
Dr. Milán Szalai, Dr. László Madácsy
Endo-Kapszula Private Medical Center, Hungary
A 36 year-old man was admitted for dysphagia, food impaction and heartburn. About 10 years ago he had clinical signs of frequent gastrooesophageal reflux, but no treatment was applied and contrast X-ray showed no pathological malformation.
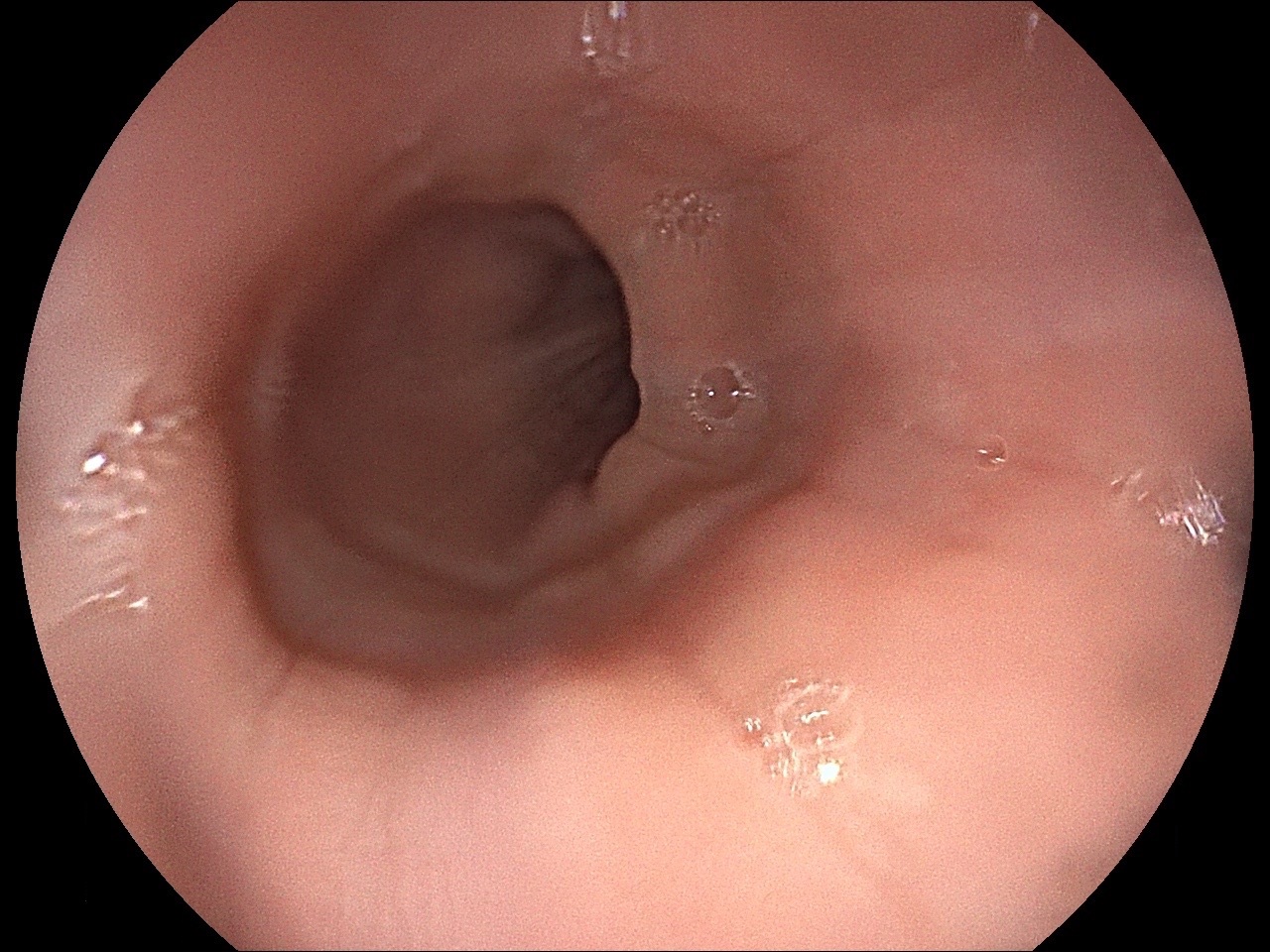
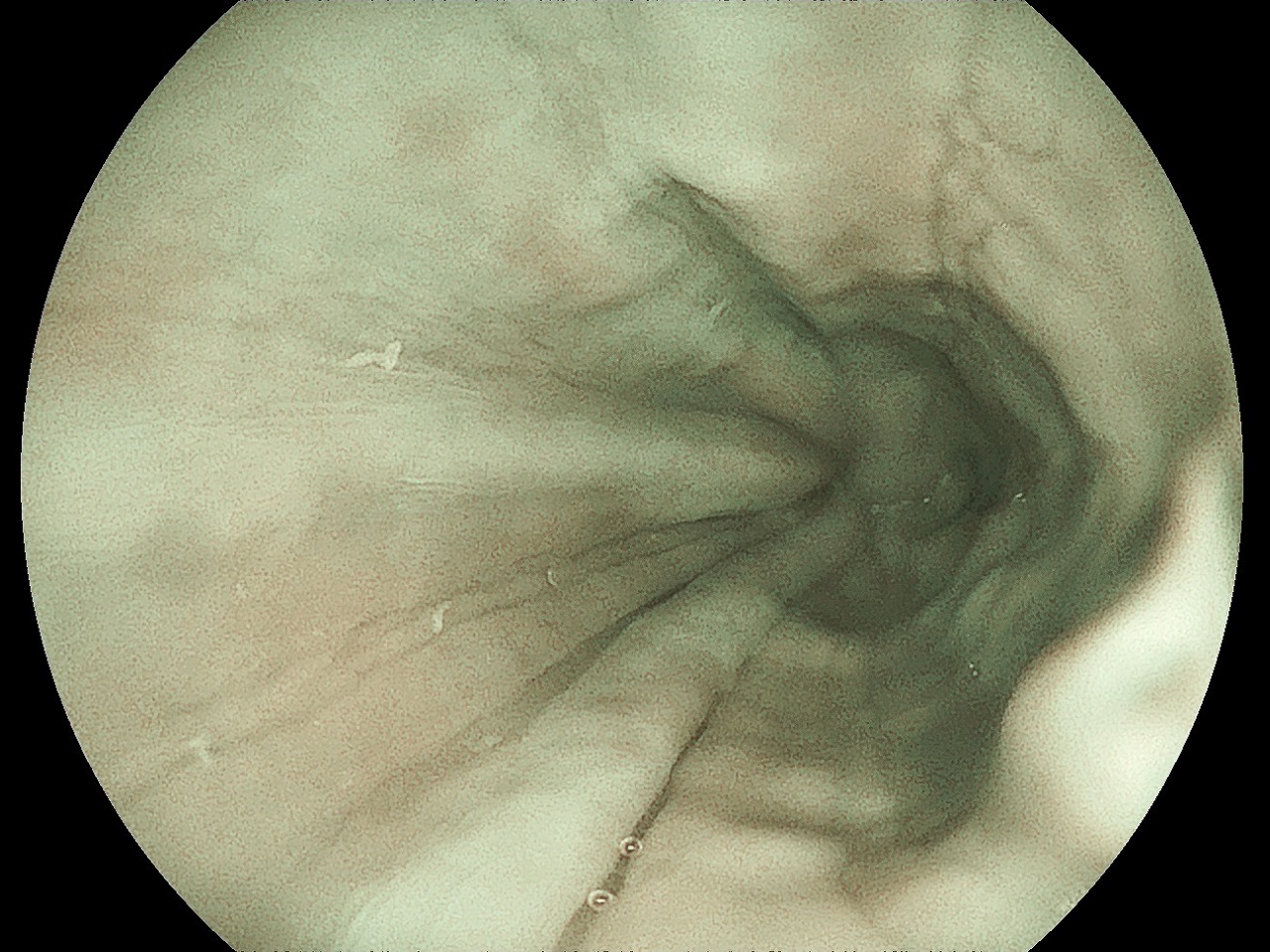
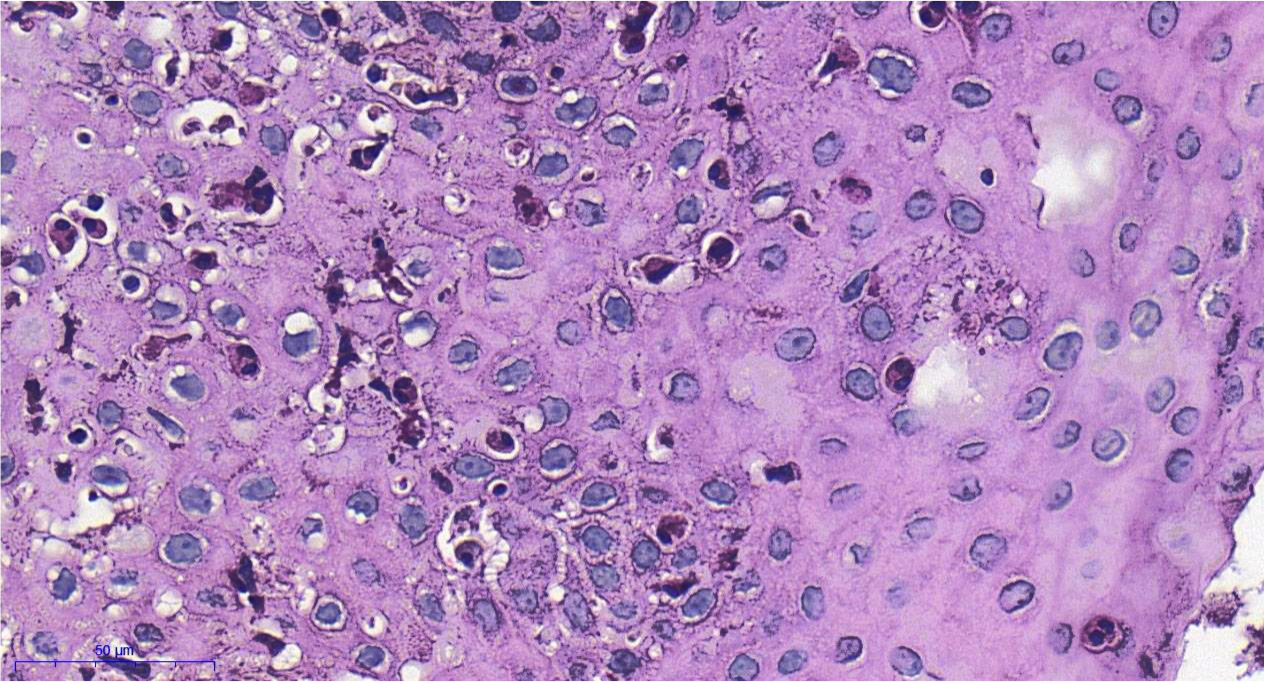
In the upper endoscopy with standard, white light imaging (WLI) no specific signs were found in the oesophagus (figure 1). However, with blue light imaging (BLI) technique obvious longitudinal furrows, concentric mucosal ring and small white plaques could be detected (figure 2). These endoscopic features raised the possibility of eosinophil oesophagitis (EoE), which was diagnosed by histological investigation (figure 3). Full-dose proton-pump inhibitor (PPI) (80 mg pantoprazol daily) and prokinetic therapy (31.6 mg metoclopramid daily) for six weeks cease the symptoms. Later, reduced dose of proton pump inhibitor therapy (20 mg pantoprazol) alone prevented the relapse.
Endoscopic features of EoE in adults include the above findings (longitudinal furrows, concentric mucosal rings, white mucosal spots) with different specificity (1,2), but these data based on with endoscopes use WLI. Obtaining biopsy specimens for the diagnosis is crucial. However, oesophageal biopsy is not a part of routine endoscopic investigation. Here, biopsy was indicated since BLI illumination (not WLI) strongly supported the presence of EoE.
EoE is an emerging clinical problem with rising incidence. It prevalence among patients presenting in endoscopy units with dysphagia is up to 15% (3). The etiology is largely unknown but food allergy related interleukin (IL) release (especially IL 5, 13, 15) seems to be important element in its pathogenesis. Reflux oesophagitis may also be a pathogenetic factor as it possibly sensitizes the mucosal layer to different allergens. In our case PPI and prokinetic therapy most probably restored the mucosal barrier and in this way prevented the further allergenic exposition and eosinophil infiltration. No other systemic treatment (e.g.: corticosteroids, montelucast) had to be applied.
References:
1. Akhondi H. Diagnostic approaches and treatment of eosinophilic esophagitis. A review article. Ann Med Surg (Lond). 2017;20:69-73. doi: 10.1016/j.amsu.2017.06.022.
2. Müller S, Pühl S, Wieth M, Stolte M. Analysis of symptoms and endoscopic findings in 117 patients with histological diagnoses of eosinophilic esophagitis. Endoscopy. 2007;39(4):339-344. DOI: 10.1055/s-2007-966216.
3. Liacouras CA, Furuta GT, Hirano I, et al. Eosinophilic esophagitis: Updated consensus recommendations for children and adults. J Allergy Clin Immunol 2011;128:3-20. http://dx.doi.org/10.1016/j.jaci.2011.02.040